Today was a good day to be at Memorial Hermann, and I couldn't have had a better return to my normal internship schedule. At 7:00, I attended a lecture with Dr. Nguyen on the pathogenesis of heart failure, given by Dr. Maximilian Buja. He presented a wealth of information about the complexities of heart disease, and much of it was completely new to me. Cardiomyocytes, the muscle cells that make up the heart, were front-and-center in his presentation; these cells are extremely powerful, and them functioning correctly is critical to the heart as a whole being able to perform. They produce ATP (basically the body's "energy currency") at an extremely quick rate, making them great at working constantly. Dr. Buja discussed the cardiomyocytes in relation to heart conditions and different diseases therein, with ischemic cardiomyopathy (ischemic CM) as one of the highlights. In ischemic CM, the heart's left ventricle is weak and can't pump blood out to the body efficiently- this is usually a result of inadequate blood supply to the heart's coronary arteries (that causes heart attacks). So, the heart tissues aren't getting enough blood/energy, which makes them unable to pump the other collections of blood through the heart's systolic chambers. One problem with the cardiomyocytes not getting enough energy is that they don't just replace themselves, and permanent damage can be done. Once the cells die, patches of necrotic tissue begin to form on the heart, and will stay until surrounding blood flow leads to the necrotic area scarring and being partially repaired. Since Dr. Buja was presenting to a room full of doctors, a lot of the above info was skipped over, so his primary focus was on the options for supporting the heart throughout ischemic CM: defibrillators, ventricle assist devices, balloon pumps, the works. There was a lot more about transplant rejection and antibody responses, but that'll take a bit to explain in detail...plus, I'm still processing that myself. Isn't learning stuff great?
Valve conference was a fairly normal length today, with a handful of cases. For those who aren't familiar with what it is, I get to watch a group of cardiologists and cardiothoracic surgeons discuss what should be done with pre-op heart patients. Powerpoints are shown, opinions differ, and occasionally, jokes are thrown around- it's generally a good time. A couple of patients had aortic stenosis (tightening of the aortic valve), a few others had coronary issues, but there was only one case that really caught my eye. There's usually one of them in every conference, a case that the doctors argue over because of its complexity or because of their individual experiences with cases like it. This one involved a 70 year old woman with symptoms of aortic stenosis, moderate mitral stenosis, and lung damage. The choice to proceed hinged on what they needed to do first, and how effective that first surgery would be in remedying the other issues. It was a quiet, well-mannered battle of aortic vs. mitral repair. One doctor chimed in to say that non-surgical procedures are what they really need to think about, because the risk is just too high to immediately consider surgery. After a lengthy discussion, I recall that they decided it was an inoperable situation; they would do the best to make the woman comfortable, but going through surgery would just be a waste of her remaining time. Being realistic is a key part of making these calls, but listening to these conversations is sobering in a world of advanced medicine. Not everyone can be saved, and the outcome won't always be great or optimal, but that's life.
That's about all I have for this week. The storyboard for the aortic stenosis project is in its second draft, and since this post is so long, I'll shorten details for the coming Friday's post and put some info/photos of it there. Whether you made it all the way through or not, thanks for reading!
Sunday, February 28, 2016
Thursday, February 25, 2016
2/24/16
Today I decided to come in to watch one of Dr. Nguyen's cases, a mini-mitral valve replacement. I didn't have any background knowledge about the patient, but being there was interesting enough; this was the first mini I've seen, and also the first operation I had seen performed on the mitral valve. The mitral valve is the first valve to be reached by oxygenated blood coming from the lungs, and is located between the left atrium and the left ventricle. A mini is a minimally-invasive surgery, which relies on 1-4 incisions around the thorax to perform the operation, as opposed to a sternotomy that splits the chest open entirely. Although there are many factors to consider, some people just don't like the recovery time involved with a sternotomy, and might pick a mini operation over it if given the choice.
The surgery starts with an incision in the lower left of the chest, near the groin; this leads directly into the femoral vein. A cannula (fancy word for tube) is inserted into the vein, and is connected to a heart-lung machine. Another cannula is drawn from the heart-lung machine to the femoral artery, creating a system that draws out blood, reoxygenates it outside of the patient, and feeds it back into the lower body. Another incision is made on the right side of the chest, just under the breast, and the hole is widened with rib spreaders. With his incision opens up a view of the pericardium, the area surrounding and holding the heart, from the ascending aorta to the diaphragm in length. The pericardium is then cut open, and sutured in place to reveal the aorta. Cardioplegia is administered- which slows and eventually stops the heart- so that the journey to the mitral valve can begin. This process is quite extensive( and definitely looks the part), as the doctor has to get all the way to the mitral valve from a hole in the pericardium. It really ends up looking like a tunnel, and gets even more confusing once the sutures and ties holding tissue in place are set. The sutures divide the tissue layers, allowing a small hole of viewing space into the mitral valve. Because of how tightly-packed the area was with sutures, clamps and cannulas, it was satisfying to be able to identify the chordae tendonae peeking out from behind the relaxed mitral valve. It was sort of like a medical version of "Where's Waldo."It was around this point that I realized that Dr. Nguyen was doing a full valve replacement. He started clipping away at the mitral valve's leaflets, and removed the valve surprisingly quickly. The replacement valve was to be mechanical, so he began attaching the sutures to the lip lining the mechanical valve, a part of one of the most complicated processes I've seen in the OR- I'm talking about the scaffolding/lowering-of-the-replacement-valve process, which secures the new valve in place. The ends of those sutures attached I wasn't able to stay to see the heart tissues sutured back together, which is a bummer, but I'm glad that I got to see most of the installation process. Because the patient received a mechanical valve, they will have to take Coumadin or Warfarin (blood thinners) daily for the rest of their lives; the structure of the mechanical valve allows blood clots to develop more easily, so this is a safety precaution.
Having seen both kinds of surgery, sternotomies and minis, sternotomies are much more appealing from the viewer's perspective. One would assume that it's easier on the doctors, too- the chest is split, and there's plenty of viewing room. It's a direct look at the heart, and all of the doctors surrounding the patient can see what is going on. Minis, on the other hand, are performed through the right of the chest, and docs assisting with the surgery have to rely on the performing doctor's live headcam footage to get a peek. I would've had no idea what was going on without Dr. Nguyen's headcam footage being projected on the nearby flatscreen TV. Even the surgical instruments involved in it are long, complicated and awkward; the highly trained professionals involved with this surgery struggled, at times, to position cannulas and other materials around the chest incision.
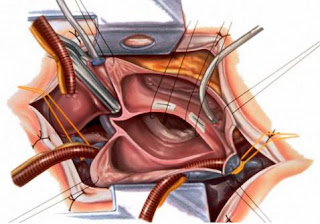
Above is a clean picture of the surgery, with clamps, cannulas, sutures and the rib spreader in place. This is still pre-valve installation
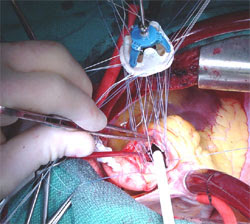
Above is a real picture (not mine) of the suture scaffolding, lowering the replacement valve in.
I thought that this deserved a long blog post, because seeing actual surgery is one of the most interesting things about this internship. The human body is incredible, and what we're able to do with it in regards to medical care is even more astonishing. Hopefully I'll be able to spectate one surgery every month or so, but because they're so long and right in the middle of the day, planning gets a bit tricky.. I'll have another post about this Friday's events (as promised) up by the end of the weekend.
The surgery starts with an incision in the lower left of the chest, near the groin; this leads directly into the femoral vein. A cannula (fancy word for tube) is inserted into the vein, and is connected to a heart-lung machine. Another cannula is drawn from the heart-lung machine to the femoral artery, creating a system that draws out blood, reoxygenates it outside of the patient, and feeds it back into the lower body. Another incision is made on the right side of the chest, just under the breast, and the hole is widened with rib spreaders. With his incision opens up a view of the pericardium, the area surrounding and holding the heart, from the ascending aorta to the diaphragm in length. The pericardium is then cut open, and sutured in place to reveal the aorta. Cardioplegia is administered- which slows and eventually stops the heart- so that the journey to the mitral valve can begin. This process is quite extensive( and definitely looks the part), as the doctor has to get all the way to the mitral valve from a hole in the pericardium. It really ends up looking like a tunnel, and gets even more confusing once the sutures and ties holding tissue in place are set. The sutures divide the tissue layers, allowing a small hole of viewing space into the mitral valve. Because of how tightly-packed the area was with sutures, clamps and cannulas, it was satisfying to be able to identify the chordae tendonae peeking out from behind the relaxed mitral valve. It was sort of like a medical version of "Where's Waldo."It was around this point that I realized that Dr. Nguyen was doing a full valve replacement. He started clipping away at the mitral valve's leaflets, and removed the valve surprisingly quickly. The replacement valve was to be mechanical, so he began attaching the sutures to the lip lining the mechanical valve, a part of one of the most complicated processes I've seen in the OR- I'm talking about the scaffolding/lowering-of-the-replacement-valve process, which secures the new valve in place. The ends of those sutures attached I wasn't able to stay to see the heart tissues sutured back together, which is a bummer, but I'm glad that I got to see most of the installation process. Because the patient received a mechanical valve, they will have to take Coumadin or Warfarin (blood thinners) daily for the rest of their lives; the structure of the mechanical valve allows blood clots to develop more easily, so this is a safety precaution.
Having seen both kinds of surgery, sternotomies and minis, sternotomies are much more appealing from the viewer's perspective. One would assume that it's easier on the doctors, too- the chest is split, and there's plenty of viewing room. It's a direct look at the heart, and all of the doctors surrounding the patient can see what is going on. Minis, on the other hand, are performed through the right of the chest, and docs assisting with the surgery have to rely on the performing doctor's live headcam footage to get a peek. I would've had no idea what was going on without Dr. Nguyen's headcam footage being projected on the nearby flatscreen TV. Even the surgical instruments involved in it are long, complicated and awkward; the highly trained professionals involved with this surgery struggled, at times, to position cannulas and other materials around the chest incision.

Above is a clean picture of the surgery, with clamps, cannulas, sutures and the rib spreader in place. This is still pre-valve installation

Above is a real picture (not mine) of the suture scaffolding, lowering the replacement valve in.
I thought that this deserved a long blog post, because seeing actual surgery is one of the most interesting things about this internship. The human body is incredible, and what we're able to do with it in regards to medical care is even more astonishing. Hopefully I'll be able to spectate one surgery every month or so, but because they're so long and right in the middle of the day, planning gets a bit tricky.. I'll have another post about this Friday's events (as promised) up by the end of the weekend.
Saturday, February 20, 2016
Update 2/19/16
Dr. Nguyen was unavailable on Friday- so, I'll probably be going early in the week. Progress is still being made on the storyboards for the animation project, and I will likely be uploading full rough draft pictures in the coming posts. I could very well be doubling up on hospital visitation next week, as I have to make up for this Friday and will be going-as per usual-next Friday morning. I'm hoping to spectate a surgery for the makeup day and have a normal morning for next Friday (valve conference, maybe a lecture, patient visits, and project updates), but that all depends on Dr. Nguyen's schedule. It'll be an interesting week regardless, so stay tuned.
Monday, February 15, 2016
2/12/15
Today was the most radical departure from my normal Friday schedule. Dr. Nguyen was busy in the morning, so I went at three in the afternoon instead. My main goal of the day was to present to him some work that I'd been doing on an animation project, but some patient drama arose just as I got there; this resulted in him rushing over to the Heart and Vascular Clinic across the street, with me in tow, to make sure that a patient's temporary pacemaker got installed. That aside, the project that I'm working on is intended to explain medical conditions in simple terms, so that a layman audience can understand what's going on. There's an entire set of jargon in medicine, and it can be quite challenging for many people to keep track of it all. I'm using aortic stenosis (the tightening of the aortic valve) as a start, developing a short story around it, and tying in an explanation of the disease. I'll probably post some images of the work, especially once we get it past the storyboarding process, but I thought this would be a good entry- as opposed to the standard blog post about some surgery or disease I just learned about.
Wednesday, February 10, 2016
2/5/16
There isn't a lot to report for today. After a very packed valve conference, Dr. Nguyen went into surgery (at around 9:30, and I had to leave at 10:20)- so I stuck with his PA for the remaining amount of time that I was there. She filled me in on the surgery that Dr. Nguyen was to perform: Valve Sparing Aortic Root Replacement. I like to call it VSARR, because that rolls off the tongue more easily, but it is also known as a David procedure. It's a pretty interesting surgery, and is quite long. If an aneurysm (air bubble) occurs in the aorta, this surgery is done to remove the aortic root, which is the area right above the aortic valve. The aorta gets clamped shut, the heart gets cooled, and the patient is put on a heart bypass machine for the duration of the surgery. Because the aortic root is so close to the coronary arteries and the aortic valve, it's hard to remove the root without doing some additional work- so, the coronary openings are detached from the aortic root, to be reattached later. This is when the aortic graft comes in. Sutures attach this piece to the aortic annulus, a structure that rings the aortic valve, and the ascending aorta above that. Finally, the coronary arteries are reattached through small holes in the graft. Variations of this surgery exist, including one that removes the aortic valve, even if there is nothing wrong with it (though, that isn't really VSARR, because it doesn't spare the valve). That specific variation is known as the Bentall Procedure. If a patient is a candidate for the David procedure, but has some aortic valve complications, they might as well go through the Bentall procedure to kill two birds with one stone. This is one of the more complicated surgeries I've learned about, although I'm sure that there are some I don't know about that are even more intricate. I really do learn something new every day that I'm here.
P.S., just to give a visual of what I was explaining:

P.S., just to give a visual of what I was explaining:

Subscribe to:
Posts (Atom)